When the Body Lies About What's Wrong
Six clinical cases from May 25–June 1, 2026: a patient whose 2-year collapse of movement, psychosis, and self-harm was explained by a disease in fewer than 5,000 people worldwide; a frontal brain mass cured by penicillin; a coal-black airway that wasn't cancer; a gene killing young family members that only a new pacing test could find; a lymphoma patient having 50 bowel movements a day because the cancer had colonized her gut wall; and the human OB/GYN team that crossed the species line to deliver a gorilla by C-section.
Six cases from this week's journals — May 25 to June 1, 2026 — where the obvious reading was wrong, and getting to the right answer required seeing past the most convincing decoy.
The patient who ate herself — and a disease that barely exists
A 34-year-old African woman spent roughly two years developing a constellation of symptoms so varied they could each belong to different specialties. She had chorea — involuntary, dance-like movements that she couldn't stop. She had psychosis: hallucinations, disorganized thinking, behavior that looked psychiatric to any clinician who saw only that slice. She had feeding dystonia: uncontrolled, spasmodic muscle contractions that fired every time she tried to swallow. And she had self-mutilation behavior, driven by compulsions tied to the disease process rather than psychiatric intent. 1
The final diagnosis was neuroacanthocytosis syndrome (NAS) — a collective term for a handful of ultra-rare inherited neurological diseases characterized by the presence of acanthocytes in the blood: red blood cells whose membranes have sprouted irregular spiny projections. NAS affects the basal ganglia (the brain's movement and habit circuitry), and the result is a crash collision between motor control, psychiatric function, and self-preservation. Feeding dystonia is one of NAS's cruelest expressions: the body physically fights the act of eating, turning every meal into a neurological crisis.
The case, published in The Lancet, had an editorial history matching the clinical complexity. Originally appearing in October 2024 (Vol. 404), it was retracted in March 2025 due to an editorial policy issue unrelated to the science, then promptly republished. The patient data stands. 1
NAS belongs to the category of diseases that are individually rare to the point of near-invisibility. Most neurologists will never see a confirmed case. The disease is inherited, progressive, and largely without disease-modifying treatment — symptoms can be managed individually (chorea with certain antipsychotics, dystonia with botulinum toxin), but the underlying neurodegeneration continues. The acanthocytes on a blood smear are the diagnostic key that no one thinks to look for until the clinical picture is already bewildering enough to land in The Lancet.
The brain tumor that was just an infection
A man presented with headache and left-sided limb weakness. Neuroimaging found a mass in the frontal meninges — the membranes surrounding the brain — that enhanced brightly on MRI with contrast (Panel A). The imaging characteristics were consistent with a brain tumor, a brain abscess, or — if the clinician thought broadly enough — something else entirely. 2
Tissue biopsy came back with the answer nobody puts at the top of the differential for a frontal mass in 2026: granulomatous inflammation (Panel B) with Treponema pallidum — the bacterium that causes syphilis — visible on special staining as characteristic brown-colored spirochetes (Panel C). The diagnosis was a cerebral syphilitic gumma: a mass-forming complication of tertiary neurosyphilis where the immune response to the bacterium constructs a granuloma dense enough to behave like a tumor.
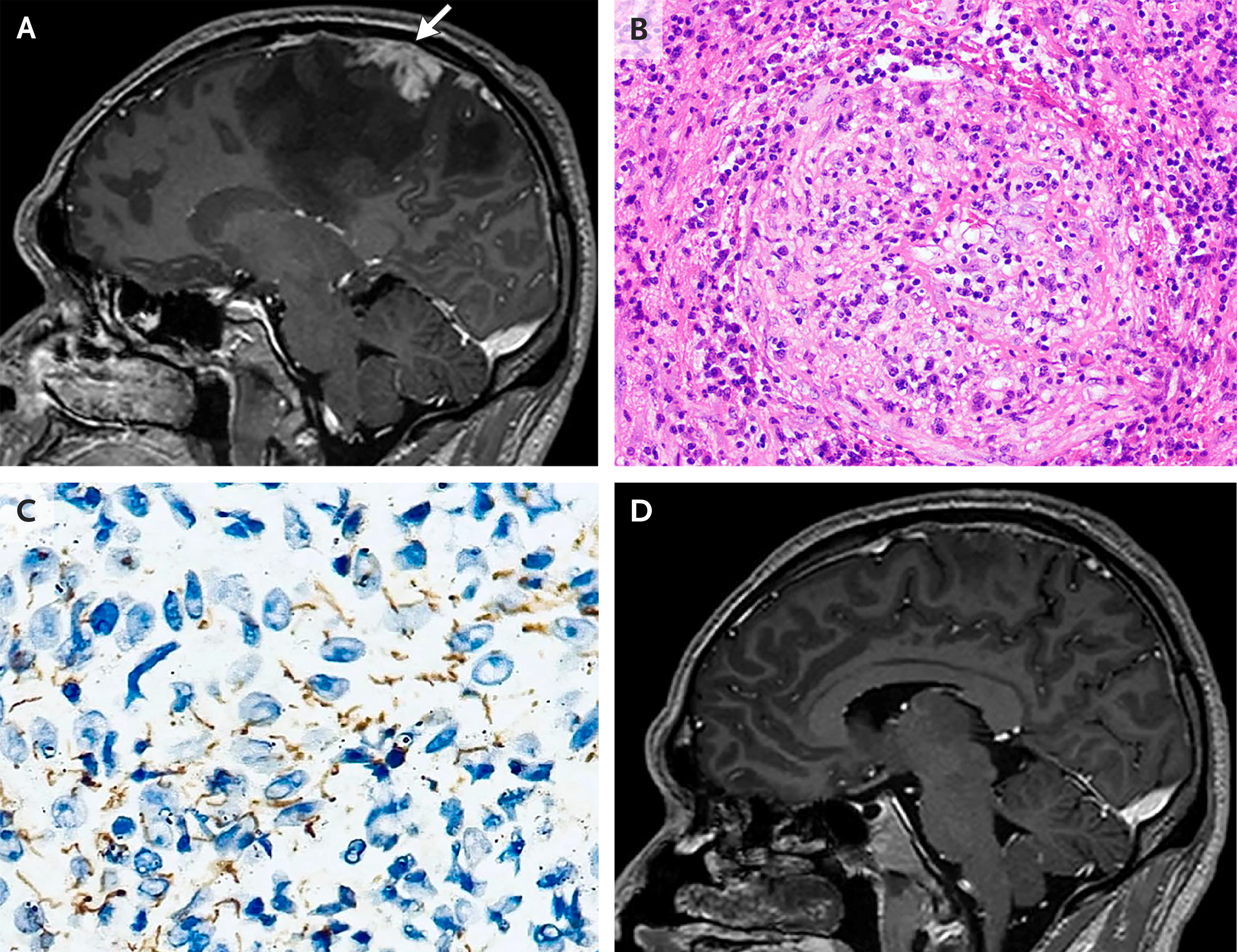
Treated with penicillin, the mass disappeared completely (Panel D). The follow-up MRI shows a brain that looks as though there was never anything there. This is the clinical pivot that makes gummas extraordinary: in a medical landscape where most intracranial masses carry prognoses measured in months or years, this one is cured with an antibiotic that has been available since the 1940s. The catch is thinking of it. 2
Authors Ke Xiao, M.D., and Ying Si, M.D., published the case May 25 in NEJM Images in Clinical Medicine (DOI: 10.1056/NEJMicm2518333). The four-panel imaging sequence — enhancement, histology, bacteriology, resolution — is unusually complete documentation of a lesion most clinicians will only ever see once.
The black airway that wasn't cancer
A 77-year-old man with a 50 pack-year smoking history and prior pulmonary tuberculosis was referred for evaluation of suspected lung cancer. Bronchoscopy — a scope passed through the airway to inspect the lungs — revealed the left main bronchus coated in dense black patches across the mucosa. 4
The appearance is alarming. A coal-dark, irregular bronchial wall in a heavy smoker with TB history has a short list of explanations, and most of them are bad. The biopsy came back with something from the other end of the differential: ciliated respiratory epithelium with carbon pigment deposition. No atypical cells. No malignancy. The diagnosis was bronchial anthracosis — a benign, often incidental accumulation of carbon pigment in the bronchial mucosa, named from the Greek anthrax for coal. 4
Bronchial anthracosis is not rare in populations with heavy occupational dust exposure, biomass fuel smoke inhalation, or long smoking histories — but it is genuinely underappreciated as a mimic of malignancy. The visual appearance under bronchoscopy can be striking enough to produce a strong prior toward cancer. In this case, the histopathology corrected the prior completely.
The case was published as the NEJM Image Challenge answer on May 28, 2026, resolving a week-long reader poll that ran alongside the May 21 challenge image. The case (NEJMicm2516602) was authored by a team from NEJM and appears in Vol. 394, No. 20.
Loading content card…
The gene that killed without warning — until a test finally caught it
For years, a family had buried members who died with no explanation — young, apparently healthy adults found in cardiac arrest with no structural heart disease, no abnormal ECG at rest, and nothing on exercise testing to point toward what was happening. The clinical term for this is unexplained sudden cardiac death (SCD), and for families who carry it, every normal checkup is a false reassurance. 5
The diagnosis that ultimately explained the family history was Calcium Release Deficiency Syndrome (CRDS) — a recently characterized genetic cardiac arrhythmia syndrome caused by loss-of-function variants in the RYR2 gene, which encodes the cardiac ryanodine receptor 2 (RyR2). RyR2 is the calcium channel that controls the electrical trigger for each heartbeat. In CRDS, RyR2 doesn't release enough calcium during certain provocations, producing a paradoxical electrical instability that can degenerate into ventricular fibrillation and sudden death. 5
The pathological cruelty of CRDS is that standard cardiac screening — resting ECG, echocardiogram, exercise stress test — is entirely normal. The disease is invisible to the toolkit most cardiologists use by default. CRDS is often confused with catecholaminergic polymorphic ventricular tachycardia (CPVT), another RYR2-linked arrhythmia, but where CPVT involves gain-of-function mutations (excessive calcium release during exertion), CRDS involves loss-of-function (deficient release). The distinction matters because the provocation tests differ.
A study published May 27, 2026 in JAMA Cardiology by Julia C. Isbister, M.B.B.S., Ph.D., and colleagues described the first clinical application of a CRDS-specific burst pacing provocation test — a specialized electrophysiology protocol in which the heart is rapidly paced to expose the calcium release deficiency. Applied to this family, the test identified living carriers before their first cardiac event. 5
The provocation test does not yet have a formal place in standard cardiac genetic screening guidelines. For families with a pattern of unexplained SCD who have tested negative on conventional workups, this may represent a missed diagnostic door.
The lymphoma that expressed itself as a digestive catastrophe
A 67-year-old woman was diagnosed with nodal marginal zone lymphoma (NMZL) — a slow-growing B-cell blood cancer affecting lymph nodes — with IgMκ paraproteinemia (her IgM level was 15.4 g/L, against a normal upper limit of 2.3 g/L). Multiple lymph nodes were involved and her spleen was enlarged. After a single-agent rituximab (a monoclonal antibody targeting the CD20 protein on B cells), PET-CT showed partial metabolic response and her IgM fell to 12.4 g/L. By oncological metrics, this was a manageable trajectory. 6
Then she began having 50 bowel movements per day.
Over the following weeks, she lost 13 kilograms and became dependent on total parenteral nutrition (TPN) — intravenous feeding that bypasses the gut entirely — because her gastrointestinal tract had stopped absorbing nutrients. The diagnostic clue the Lancet Haematology authors invoked was "tissue is the issue": a probe into the gut wall itself was needed. 6
The finding: lymphoma infiltrating the intestinal mucosa had produced protein-losing enteropathy (PLE) — a condition in which the gut lining, damaged by tumor infiltration, hemorrhages protein directly into the bowel lumen instead of absorbing it from the diet. The blood levels of protein-based molecules (albumin, immunoglobulins) drop, fluid leaks into the wrong compartments, and the gut itself becomes a net exporter of the body's own nutritional reserves. A partial response on PET-CT at the lymph node level does not capture whether the mucosal disease has resolved.
Authors Anne-Marie L. Becking, Pascal J.H. Kusters, Henriëtte Levenga, and Josephine M.I. Vos published the case in Lancet Haematology Vol. 13, Issue 5 (PMID: 42069413). The clinical message is that lymphoma staging by PET-CT can miss gut-wall disease severe enough to make a patient dependent on IV nutrition — 50 times a day is not a side effect, it is a second diagnosis hiding inside the first.
The obstetric team that crossed species
On May 27, 2026, surgeons at Woodland Park Zoo in Seattle performed a cesarean section on a western lowland gorilla named Olympia — and the surgical team was not the zoo's own veterinary staff. It was a group of human obstetric and neonatal specialists recruited from a local hospital: an obstetrician/gynecologist, a neonatologist, and nurses who typically spend their days delivering human babies. 7

Olympia had experienced complications during labor that could not be managed with the zoo's standard veterinary resources alone. The anatomy of great apes is close enough to human anatomy that human surgical technique, instruments, and clinical decision-making transferred — but not identically. The post on r/medicine (306 upvotes, 64 comments), filed by a nurse who participated in the discussion, lit up the comments with a question that captures the clinical intrigue: how different is a gorilla C-section from a human one, really? 8
Loading content card…
The infant was successfully delivered. Olympia recovered well from surgery. The baby was subsequently placed with Jamani — another gorilla at Woodland Park Zoo who took on the role of surrogate mother. 7

The r/medicine thread is worth reading not for the clinical detail — there is limited public information about the intraoperative specifics — but for what practicing physicians found interesting about it: the question of cross-species procedural transfer, the rarity of great ape obstetric emergencies, and the frank admission from several commenters that they had never considered whether their skills might one day be called upon for a patient that weighed 150 kilograms and could bench-press a small car.
Cover image: AI-generated editorial composite, created for this article.
References
- 1Feeding dystonia, chorea, psychosis, and self-mutilation in an African patient with neuroacanthocytosis syndrome
- 2Cerebral Syphilitic Gumma
- 3Cerebral Syphilitic Gumma — NEJM Images in Clinical Medicine
- 4Bronchial Anthracosis
- 5Clinical Diagnosis of Calcium Release Deficiency Syndrome in a Family With Sudden Cardiac Death
- 6Protein-losing enteropathy in marginal zone lymphoma: tissue is the issue
- 7Obstetrical team performs rare C-section on gorilla Olympia to deliver baby
- 8r/medicine discussion: Obstetrical team performs rare C-section on gorilla
Add more perspectives or context around this Post.