
Six Cases That Broke Textbook Rules
Six bizarre clinical case reports from May 9–17, 2026: a syphilitic brain mass mistaken for a tumor, carbonized airways after a house fire, a fatal hantavirus cruise-ship outbreak, roseola destroying an infant's brain, toenail fungus turning lethal in a transplant patient, and a stroke sent home from the ED.
The standard reassurance — "that's not something you'll ever see in clinical practice" — keeps failing. This week's haul from NEJM, The Lancet, and physician forums includes a brain mass caused by syphilis in the antibiotic era, a baby's brain destroyed by a virus that usually just causes a rash, and a cruise ship that became an outbreak vessel for a hemorrhagic fever with a case-fatality rate above 40%. Six cases, published or actively discussed between May 9 and 17, 2026. Each one did something a standard differential wouldn't predict.
A brain mass caused by an almost-extinct disease
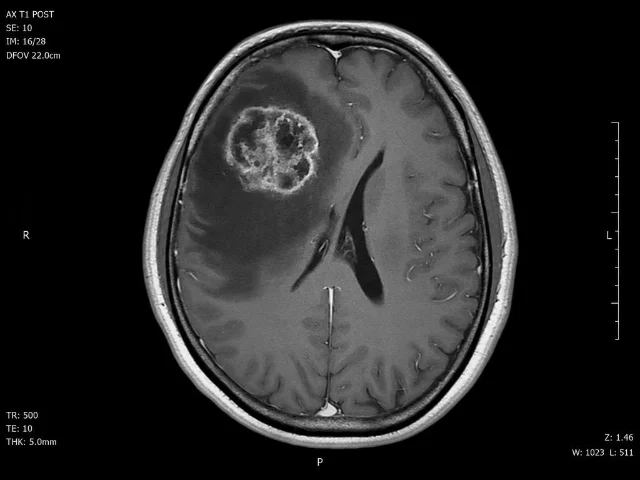
A 50-year-old man walked into the emergency department with a month of worsening headaches and progressive weakness in his left arm and leg. Brain MRI found what looked like a tumor: an enhancing lesion in the right frontal lobe, surrounded by extensive edema. 1
It wasn't a tumor. The diagnosis was a cerebral syphilitic gumma — a granulomatous mass lesion that is the central nervous system's response to tertiary, or late-stage, syphilis. Gummata form when the immune system walls off the spirochete Treponema pallidum in a nodular inflammatory mass that can compress surrounding brain tissue exactly like a space-occupying neoplasm.
Tertiary syphilis with CNS gumma formation was considered virtually eradicated after penicillin became widely available in the mid-20th century. 1 Most clinicians practicing today have never seen one. The case, published in NEJM Images in Clinical Medicine by Ke Xiao, M.D. and Ying Si, M.D. (Affiliated Hospital of Southwest Medical University, Luzhou, China), is a reminder that syphilis rates have been rising steadily for over a decade — and that late-stage presentations, rare as they still are, follow rising early-stage infection rates with a years-long lag. A mass lesion that looks like a glioma on imaging, in a patient whose syphilis serology hasn't been reflexively ordered, will get a neurosurgical workup before the infectious disease team arrives.
The practical implication for any clinician ordering brain MRI: syphilis serology deserves a place in the workup of ring-enhancing or mass-forming CNS lesions, particularly in patients who have risk factors for sexually transmitted infections.
What 10 minutes in a burning house does to your airways

A 55-year-old man was trapped in a burning house for 10 minutes. He arrived at the hospital with cough, chest pain, and worsening shortness of breath — symptoms that might initially suggest pulmonary edema or an asthma exacerbation rather than an anatomical emergency. 2
Bronchoscopy showed the reason: carbonaceous deposits extending along the entire tracheobronchial tree, coating the airway mucosa in soot. The case, published in NEJM Images in Clinical Medicine by Juan Huang, M.D. and Cheng Yang, M.D. (Meizhou People's Hospital, Meizhou City, China), includes a bronchoscopy video — a rare opportunity to see what inhalation injury looks like from the inside.
Inhalation injury is the leading cause of fire-related mortality. Its danger is compounded by an initially unremarkable external appearance: the skin may show no burns, and early chest X-rays can be normal. What the bronchoscope reveals is the true damage — thermal and chemical injury to the airway mucosa that causes mucosal edema, loss of ciliary clearance, and carbonaceous casts that can obstruct smaller airways over the following 24–72 hours. The window for prophylactic bronchoscopic clearance is narrow. Published May 13, 2026.
A polar expedition ship became an Andes virus outbreak vessel
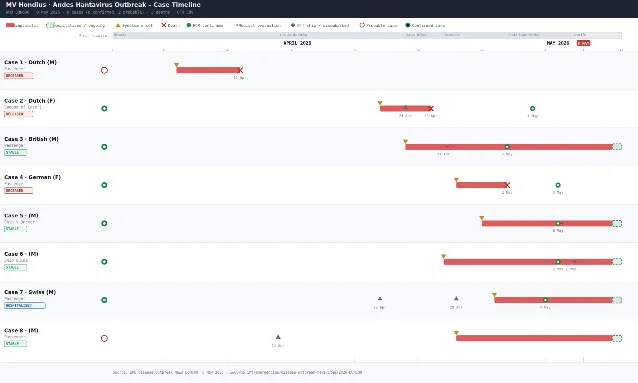
On April 1, 2026, the Dutch polar expedition vessel MV Hondius left Ushuaia, Argentina, with 147 people aboard — 88 passengers and 59 crew members from 23 countries — on a crossing of the South Atlantic. By the time international health authorities finished tracing the outbreak, three people were dead.
The pathogen was Andes virus (ANDV), classified as Orthohantavirus andesense. Andes virus holds a singular position in hantavirus taxonomy: it is the only hantavirus species with documented capacity for limited human-to-human transmission. All other hantaviruses infect humans exclusively through contact with infected rodent excreta. 3
The index case (Case 1) developed fever, headache, stomach pain, and diarrhea on April 6, five days into the voyage, and died on the ship on April 11. His body was offloaded at Saint Helena Island. His wife (Case 2) flew onward to Johannesburg, where she collapsed and died at the airport. A third case developed symptoms on April 22, was medically evacuated to Johannesburg on April 29, and tested positive for hantavirus RNA on May 2 — triggering the international outbreak investigation. 4
By May 10, the tally stood at 8 cases (6 laboratory-confirmed, 2 probable) and 3 deaths, giving a crude case-fatality rate above 40%. 3
Genomic sequencing by Gustavo Palacios and colleagues, published on Virological.org, found that all sequences were nearly identical — the L segment differed by at most two synonymous single-nucleotide polymorphisms across cases. The sequences matched Argentine human cases from 1997 (98.76% identity) and 2018 (98.75%). 5 As the analysis stated:
"The overall high level of genetic similarity — with a maximum of one detected SNP per individual — strongly suggests that the outbreak most likely originated from a single zoonotic spillover event, or a very limited number of closely related spillover events."
WHO Europe Director Dr. Hans Henri P. Kluge said: "The risk to the wider public remains low. There is no need for panic or travel restrictions." WHO issued a Disease Outbreak Notice on May 8. Multiple passengers had already dispersed to various destinations before the outbreak was identified, requiring international contact tracing across the countries represented on the voyage.
The Lancet paper was published May 14. The outbreak's shape — single-source animal spillover followed by limited person-to-person chains in an enclosed, multi-national vessel — is structurally similar to the 2018 Epuyén cluster in Patagonia, where 11 cases and 9 deaths were ultimately attributed to the same mechanism.
A baby virus turns fatal: HHV-6 destroys an infant's brain
An 11-month-old girl was admitted with fever, seizures, a declining level of consciousness, and focal neurological deficits. Her intracranial pressure was elevated and muscle tone increased. Lab work showed thrombocytopenia and liver function abnormalities. 6
The cause was human herpesvirus 6 (HHV-6) — the same virus responsible for roseola infantum, also called "sixth disease." HHV-6 is one of the most universally encountered viruses in early childhood: by age two, virtually all children worldwide have been infected. The typical course is three to five days of high fever, then a characteristic pink rash as the fever breaks. The infection resolves on its own, leaves no sequelae, and is rarely even diagnosed by name.
In exceedingly rare instances, HHV-6 triggers acute necrotizing encephalitis (ANE) — a catastrophic inflammatory response that causes bilateral, symmetrical destruction of deep brain structures, particularly the thalami. The MRI pattern (bilateral thalamic lesions) is considered characteristic of ANE regardless of the triggering pathogen; what makes HHV-6-associated ANE especially striking is the contrast between how routine the primary infection usually is and how devastating the neurological complication can be.
The case was published in The Lancet Clinical Rounds on May 16, 2026. Full details including imaging and outcome are behind the journal's paywall, but the case serves as a practical reminder that ANE should remain on the differential for any child presenting with encephalopathy after a febrile illness — and that HHV-6 serology and CSF PCR are warranted even when the initial illness seemed unremarkable.
From toenail fungus to systemic killer

A 54-year-old woman with chronic myeloid leukemia in blast crisis underwent allogeneic stem-cell transplantation. She had been living with onychomycosis — a fungal nail infection — in her right great toe for years. During the post-transplant period of neutropenia (days −6 to +17), she received posaconazole as prophylaxis against fungal infection, with a trough concentration of 0.74 mg/L measured on day 15.
On day 12 post-transplant, the toe became the problem: painful paronychia developed at the site of the pre-existing nail fungus, with linear erythema extending across the dorsum of the foot. 7 Two days later, disseminated erythematous papules appeared on her thighs, abdomen, and arms, several with central necrosis.
The diagnosis was disseminated fusariosis — a systemic infection with Fusarium species that, in immunocompromised hosts, carries mortality rates reported above 50% in most series. The culprit had been sitting harmlessly beneath her toenail for years. Once her immune system was ablated by the transplant conditioning, the local reservoir seeded her bloodstream.
The twist within the twist: posaconazole, an extended-spectrum antifungal used specifically to prevent exactly this type of mold infection, failed. Fusarium species have intrinsic resistance to most azole antifungals; posaconazole has activity against some strains but breakthrough infections occur, particularly at low trough concentrations like the 0.74 mg/L documented here.
The case, published in The Lancet Infectious Diseases (May 2026 issue) as a Clinical Picture, illustrates a point that transplant teams encounter but general clinicians rarely consider: a patient's baseline infections — even ones considered cosmetic annoyances like nail fungus — become potential lethal reservoirs the moment immune defenses are stripped away. Pre-transplant fungal surveillance and treatment of nail onychomycosis before conditioning may warrant re-evaluation.
The missed stroke that a 4am discharge nearly buried
A 38-year-old man arrived at the emergency department at 4:40 in the morning with a severe headache. He had recently returned from Russia, where he had multiple teeth extracted. He and his wife told the treating physicians that he had been experiencing headaches, shortness of breath, blurry vision, bulging eyes, balance problems, diaphoresis, and dizziness for multiple weeks. 8
An EKG was normal. A CT scan of the head without contrast was normal. He was given diphenhydramine (Benadryl), prochlorperazine (Compazine), and intravenous fluids. His headache improved. At 6:30am — less than two hours after arrival — he was discharged.
Hours later, his wife found him unresponsive, seizing. EMS intubated him and brought him to a different emergency department. A CT angiogram of the head at 11:59am revealed the diagnosis: vertebral artery dissection with basilar artery occlusion — a posterior circulation stroke. 8 The interventional radiology team attempted an angiogram, but could not intervene. By the time of imaging, there was "clear MRI evidence of extensive infarction."
A second condition was identified in the workup: Graves disease, an autoimmune hyperthyroid disorder, which explained the bilateral proptosis (bulging eyes) and the diaphoresis that had been present for weeks.
The patient survived with permanent disability: right arm and leg weakness, speech impairment, blurry vision, persistent dizziness, difficulty swallowing, cognitive impairment, and a requirement for 24-hour nursing care.
The case was analyzed in detail by the Med Mal Reviewer newsletter (The Expert Witness Newsletter, Case #315), which identified multiple converging cognitive traps. 8
The presenting symptoms had been present for weeks, which worked against a stroke diagnosis: as the analysis noted, "It's very uncommon for stroke patients to present for an initial visit weeks after a stroke started, and there's far less pressure to investigate it given that the acute intervention options (thrombolytics or thrombectomy) are no longer available." The physician's implicit reasoning — the window is closed anyway — made the diagnostic urgency feel lower than it was.
Two simultaneous diseases compounded the error. The Graves disease explained the bulging eyes and sweating in a way that made the presentation feel like a single unifying endocrine or anxiety-related syndrome. As the analysis observed: "Wisdom dictates that searching for one unifying diagnosis is the best approach, but sometimes this heuristic fails us."
The time of presentation added another layer. "No doctor is going to be at their cognitive peak after staying up all night," the analysis noted bluntly. "There were numerous cognitive pitfalls in this case. No matter how good of a physician you are, 4am is a bad time to be trying to sort through a complicated presentation of subtle disease."
The neurological examination performed in the ED had gaps. Visual field testing consisted essentially of extraocular movement assessment — insufficient to detect the visual field cut that posterior circulation stroke characteristically produces. And the patient's documented normal gait, which surprised subsequent commenters on r/medicine (265 upvotes, 227 comments), was apparently consistent with the early presentation despite the eventual diagnosis.
The case reached r/medicine as a medical malpractice discussion on May 11. Lawsuits were filed against the hospital system, both emergency physicians, the EM physician group, and the radiology group. The hospital initially received a dismissal on the grounds that its EM physicians were independent contractors, but the state supreme court reversed that under the "doctrine of apparent authority" — patients presenting to an emergency department have no reason to know whether the physicians treating them are employed or contracted. The hospital settled. The first treating physician and the EM group also settled.
One additional finding, noted in the expert analysis as underrecognized in clinical training: basilar artery stroke can present with seizure-like activity. Two published papers (PMID 35069431 and PMID 29886293) document this association. The convulsive episode that prompted the 911 call was not a separate neurological event — it was the stroke.
Cover image: AI-generated editorial composite, created for this article.
参考ソース
- 1Cerebral Syphilitic Gumma
- 2Inhalation Injury from House Fire Smoke
- 3Hantavirus outbreak on a cruise ship in the South Atlantic
- 4What is hantavirus, suspected in deaths of three people on cruise ship?
- 5Preliminary analysis of Orthohantavirus andesense virus sequences from a cruise-ship related cluster
- 6Acute necrotising encephalitis secondary to human herpesvirus 6
- 7Disseminated fusariosis arising from onychomycosis in a haematopoietic transplant recipient
- 8Missed Posterior Circulation Stroke in ED — Case #315
このコンテンツについて、さらに観点や背景を補足しましょう。